
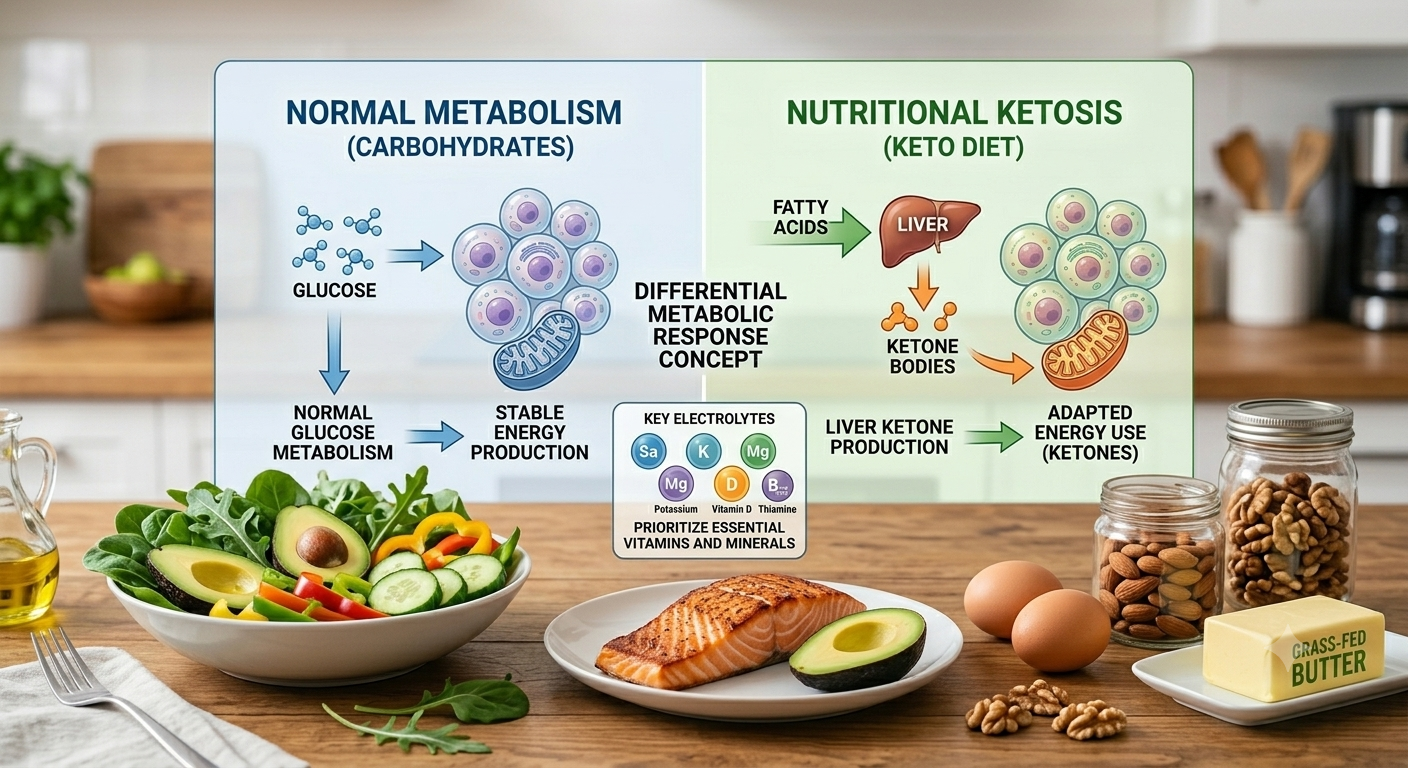
The ketogenic diet — commonly called "keto" — is a high-fat, very low-carbohydrate eating pattern that fundamentally changes the way your body produces and uses energy. Under normal circumstances, the body relies on glucose (sugar) derived from carbohydrates as its primary fuel. When carbohydrate intake is drastically reduced to roughly 20–50 grams per day, and fat intake is substantially increased to account for approximately 70–80% of total calories, the liver begins converting fatty acids into molecules called ketone bodies — specifically beta-hydroxybutyrate, acetoacetate, and acetone. This metabolic state is known as nutritional ketosis. Protein intake is kept moderate, typically around 15–20% of total calories, because excess protein can be converted to glucose through a process called gluconeogenesis, which can disrupt ketosis. Originally introduced in the 1920s as a medical treatment for epilepsy, the ketogenic diet has since become one of the most extensively studied dietary interventions in modern medicine.
The ketogenic diet centers on foods that are naturally rich in healthy fats and very low in carbohydrates. The following categories are generally encouraged:
The emphasis is on whole, minimally processed foods that provide satiety and nutritional density without pushing carbohydrate intake above the threshold needed to maintain ketosis.
Because even moderate amounts of carbohydrates can disrupt ketosis, a wide range of common foods must be significantly limited or eliminated entirely:
Reading food labels carefully is essential, as carbohydrates are hidden in many packaged and processed foods that might not appear obviously sweet or starchy.
The ketogenic diet has been investigated across a growing number of clinical contexts. The following represent areas with the most substantial published evidence:
Epilepsy
The strongest and most established evidence supports the ketogenic diet as a treatment for drug-resistant epilepsy, particularly in children. A landmark randomized controlled trial published in The Lancet Neurology found that after three months, 38% of children following the ketogenic diet experienced more than a 50% reduction in seizure frequency, compared to only 6% of controls. Updated clinical guidelines from the International Ketogenic Diet Study Group continue to recommend this dietary approach as a well-validated therapeutic option for refractory epilepsy.
Type 2 Diabetes and Blood Sugar Control
A growing body of high-quality research demonstrates that the ketogenic diet can significantly improve blood sugar regulation in individuals with type 2 diabetes (T2DM) or prediabetes. A randomized crossover study published in The American Journal of Clinical Nutrition enrolled 40 adults with prediabetes or T2DM who followed both a well-formulated ketogenic diet and a Mediterranean-style diet for 12 weeks each. Both diets improved glycated hemoglobin (HbA1c), though the ketogenic diet produced more consistent reductions in fasting insulin and triglycerides. A 2024 systematic review and meta-analysis published in Nutrition and Metabolism, which analyzed 29 clinical trials through March 2024, found that adherence to a very low-carbohydrate ketogenic diet was associated with significant reductions in fasting blood glucose, HbA1c, insulin resistance (HOMA-IR), and triglycerides compared to standard dietary recommendations.
The ketogenic diet has been compared to conventional calorie-restricted diets in numerous clinical trials. A pragmatic randomized controlled trial published in Nutrients compared a healthy ketogenic diet (net carbohydrates ≤50 g/day) to a standard energy-restricted diet in 80 adults with obesity over six months. The ketogenic group achieved greater reductions in body weight, body mass index, and visceral fat, with favorable effects on triglycerides and insulin sensitivity. These findings align with a 2022 meta-analysis published in the International Journal of Environmental Research and Public Health, which pooled data from randomized controlled trials and found that ketogenic diets produced greater improvements in weight, glycemic control, and lipid profiles in overweight individuals with T2DM compared to control diets.
Nonalcoholic Fatty Liver Disease (NAFLD)
Nonalcoholic fatty liver disease (NAFLD) — now also referred to as metabolic dysfunction-associated steatotic liver disease (MASLD) — affects an estimated 30–38% of the global population and is strongly linked to insulin resistance, obesity, and metabolic syndrome. The ketogenic diet has attracted increasing research interest as a dietary intervention for this condition. Luukkonen and colleagues (2020), in a mechanistic study published in the Proceedings of the National Academy of Sciences, demonstrated that just six days of a ketogenic diet reduced intrahepatic triglyceride content by 31% and decreased hepatic insulin resistance by 58% in individuals with NAFLD, despite a modest 3% reduction in body weight — suggesting the metabolic effect goes beyond weight loss alone. Tendler and colleagues (2007), in an earlier pilot study published in Digestive Diseases and Sciences, placed five patients with biopsy-confirmed NAFLD on a low-carbohydrate ketogenic diet for six months. At follow-up liver biopsy, four of the five patients showed meaningful reductions in hepatic steatosis, necroinflammation, and a trend toward improved liver fibrosis. A 2024 review in the Journal of Clinical Medicine summarized the current evidence and concluded that the ketogenic diet addresses multiple underlying drivers of NAFLD simultaneously, including reducing de novo lipogenesis (the liver’s own fat production), improving insulin signaling, and promoting fat oxidation through ketogenesis.
Neurological Conditions
Researchers are exploring the role of nutritional ketosis in conditions such as Alzheimer's disease, Parkinson's disease, and traumatic brain injury, based on the brain's ability to utilize ketone bodies as an alternative energy source when glucose metabolism is impaired. A randomized, double-blind, placebo-controlled multicenter trial showed that a ketogenic medical food improved cognitive function in some Alzheimer's patients — particularly those without the APOE4 genetic variant. This remains an active and evolving area of investigation.
The ketogenic diet is being studied as an adjunct to conventional cancer treatment, based on the observation that many cancer cells preferentially rely on glucose for energy (known as the Warburg effect) and may be metabolically disadvantaged in a ketotic state. A 2025 systematic review and meta-analysis published in Frontiers in Nutrition pooled results from multiple randomized and controlled trials in cancer patients and found that a ketogenic diet significantly reduced fat mass, visceral fat, insulin levels, blood glucose, fatigue, and insomnia compared to non-ketogenic diets, while also improving cholesterol levels, thyroid function markers, and emotional and social wellbeing. The review noted that benefits on inflammatory markers were more pronounced when the diet was followed for longer than 12 weeks. While these findings are encouraging — particularly for quality of life and metabolic health during cancer treatment — the effect of the ketogenic diet on tumor progression itself remains inconsistent across studies, and larger, longer-term trials are still needed before firm clinical recommendations can be made. Anyone considering this approach during active cancer treatment should do so only under close supervision of their oncology team.
Potential Side Effects
While the ketogenic diet is considered safe for most healthy adults under appropriate supervision, it is not without potential adverse effects. Being aware of these allows individuals to prepare and manage them more effectively.
The most commonly reported short-term experience is often called the "keto flu" — a collection of symptoms including headache, fatigue, mental fog, irritability, nausea, and muscle cramps that typically appear during the first one to two weeks, as the body adapts to using fat rather than glucose for fuel. These symptoms are largely driven by rapid fluid and electrolyte losses that occur when insulin levels drop and the kidneys begin excreting more sodium. Adequate fluid intake and electrolyte supplementation substantially reduce these symptoms for most people.
Other potential concerns include constipation (due to the reduced fiber intake that results from eliminating whole grains, most fruits, and legumes), elevated LDL cholesterol in some individuals, and kidney stones — particularly in children using the diet therapeutically for epilepsy. In rare cases — especially in individuals with underlying metabolic conditions — a dangerous state called diabetic ketoacidosis can develop, though this is distinct from the safe nutritional ketosis the diet aims to produce. Because the diet restricts entire food groups, micronutrient deficiencies are a real risk if the diet is not carefully planned. Long-term adherence also remains a practical challenge for many individuals, and the ketogenic diet may be contraindicated in those with pancreatitis, advanced liver disease (such as cirrhosis), or inherited disorders of fat metabolism, without close medical supervision.
A particularly important warning involves the gallbladder. The high fat content of the ketogenic diet requires the gallbladder to release more bile to help digest and absorb that fat, and the rapid weight loss that is common in the early months of the diet can further alter bile composition and gallbladder motility. Together, these factors can increase the risk of gallstone formation or trigger symptoms in individuals who already have gallstones, including right-sided upper abdominal pain, nausea, and discomfort after fatty meals. Anyone with a history of gallstones, prior gallbladder removal, or new abdominal pain after starting the ketogenic diet should discuss this with their healthcare provider, as dietary adjustments or further evaluation may be needed.
Because the ketogenic diet restricts or eliminates many food groups, certain vitamins and minerals are at heightened risk of depletion. The following supplements are most commonly recommended based on available evidence:
Primary References
. Neal, E. G., Chaffe, H., Schwartz, R. H., Lawson, M. S., Edwards, N., Fitzsimmons, G., Whitney, A., & Cross, J. H. (2008). The ketogenic diet for the treatment of childhood epilepsy: A randomised controlled trial. The Lancet Neurology, 7(6), 500–506. https://doi.org/10.1016/S1474-4422(08)70092-9
Kossoff, E. H., Zupec-Kania, B. A., Auvin, S., Ballaban-Gil, K. R., Bergqvist, A. G. C., Blackford, R., Buchhalter, J. R., Caraballo, R. H., Cross, J. H., Dahlin, M. G., & Wirrell, E. C. (2018). Optimal clinical management of children receiving dietary therapies for epilepsy: Updated recommendations of the International Ketogenic Diet Study Group. Epilepsia Open, 3(2), 175–192. https://doi.org/10.1002/epi4.12225
Gardner, C. D., Landry, M. J., Perelman, D., Petlura, C., Kernel, E., Dahl, W. J., Sonnenburg, J., & Kim, S. H. (2022). Effect of a ketogenic diet versus Mediterranean diet on glycated hemoglobin in individuals with prediabetes and type 2 diabetes mellitus: The interventional Keto-Med randomized crossover trial. The American Journal of Clinical Nutrition, 116(3), 640–652. https://doi.org/10.1093/ajcn/nqac154
Al-Hamdan, R., Almasud, M., Almatrafi, A., Alqahtani, A., Almadani, K. H., Alfaraj, A. H., & Al-Ayed, M. (2024). Impact of very low carbohydrate ketogenic diets on cardiovascular risk factors among patients with type 2 diabetes: GRADE-assessed systematic review and meta-analysis of clinical trials. Nutrition and Metabolism, 21(1), 54. https://doi.org/10.1186/s12986-024-00824-w
. Lim, S. L., Tay, M., Ang, S. M., Wai, S. N., Ong, K. W., Neo, W. J., Yap, Q. V., Chan, Y. H., & Khoo, C. M. (2024). Development and pragmatic randomized controlled trial of healthy ketogenic diet versus energy-restricted diet on weight loss in adults with obesity. Nutrients, 16(24), 4380. https://doi.org/10.3390/nu16244380
Zhou, C., Wang, M., Liang, J., He, G., & Chen, N. (2022). Ketogenic diet benefits to weight loss, glycemic control, and lipid profiles in overweight patients with type 2 diabetes mellitus: A meta-analysis of randomized controlled trials. International Journal of Environmental Research and Public Health, 19(16), 10429. https://doi.org/10.3390/ijerph191610429
Luukkonen, P. K., Dufour, S., Lyu, K., Zhang, X. M., Hakkarainen, A., Lehtimäki, T. E., Cline, G. W., Petersen, K. F., Shulman, G. I., & Yki-Järvinen, H. (2020). Effect of a ketogenic diet on hepatic steatosis and hepatic mitochondrial metabolism in nonalcoholic fatty liver disease. Proceedings of the National Academy of Sciences, 117(13), 7347–7354. https://doi.org/10.1073/pnas.1922344117
Tendler, D., Lin, S., Yancy, W. S., Mavropoulos, J., Sylvestre, P., Rockey, D. C., & Westman, E. C. (2007). The effect of a low-carbohydrate, ketogenic diet on nonalcoholic fatty liver disease: A pilot study. Digestive Diseases and Sciences, 52(2), 589–593. https://doi.org/10.1007/s10620-006-9433-5
Dyńka, D., Rodzeń, Ł., Rodzeń, M., Łojko, D., Kraszewski, S., Ibrahim, A., Hussey, M., Deptuła, A., Grzywacz, Ż., Ternianov, A., & Unwin, D. (2024). Beneficial effects of the ketogenic diet on nonalcoholic fatty liver disease (NAFLD/MAFLD). Journal of Clinical Medicine, 13(16), 4857. https://doi.org/10.3390/jcm13164857
Henderson, S. T., Vogel, J. L., Barr, L. J., Garvin, F., Jones, J. J., & Costantini, L. C. (2009). Study of the ketogenic agent AC-1202 in mild to moderate Alzheimer’s disease: A randomized, double-blind, placebo-controlled, multicenter trial. Nutrition and Metabolism, 6, 31. https://doi.org/10.1186/1743-7075-6-31
Zhang, M., Zhang, Q., Huang, S., Lu, Y., & Peng, M. (2025). Impact of ketogenic diets on cancer patient outcomes: A systematic review and meta-analysis. Frontiers in Nutrition, 12, 1535921. https://doi.org/10.3389/fnut.2025.1535921


